AdsTalk 25 with Dr Zoe Picton-Howell
Dr Zoe Picton-Howell, solicitor, academic, expert in healthcare law and ethics and Adam’s mother gave the 10th anniversary Adam Bojelian Foundation talk on 31st March 2025 entitled: Law as the catalyst for optimum patient care and staff well-being- not fear’.
 You can access a video of Zoe talk here: AdsTalk25 -Law as the catalyst for optimum patient care and staff well-being – not fear
You can access a video of Zoe talk here: AdsTalk25 -Law as the catalyst for optimum patient care and staff well-being – not fear
The following is the full text of Zoe’s talk:
The 2025 Adam Bojelian Memorial Talk
“Law as the Catalyst for Optimum Patient Care and Staff Well-being—Not Fear”
Introduction
Hello and welcome to the 2025 Adam Bojelian Memorial Talk. The theme for this year is “Law as the Catalyst for Optimum Patient Care and Staff Well-being—Not Fear.”
Thank you all for being here, especially those who have travelled a significant distance to join us. This is a deeply personal talk for me, and as such, I will be using notes—so please forgive me if I occasionally look down at them.
I will speak for about an hour, and this talk is being recorded by Paul for those unable to attend today. After the talk, we will switch off the recording to allow for open and candid questions and discussion about the issues raised.
Honouring Adam Bojelian
This talk is held in loving memory of Adam Bojelian, who died ten years ago this month at just 15 years old—far too soon. Since his death, apart from 2020 when the pandemic forced its cancellation, the Adam Bojelian Memorial Talks have been held annually. I extend my gratitude to all who have supported these talks over the years, whether by giving, chairing, attending, promoting, or sharing them. A special thank you to Horizon Leeds for generously hosting us today.
I will speak more about Adam shortly, but first, I want to reflect on why these talks began. Despite his young age, Adam was widely recognised by senior NHS staff for his remarkable contributions to healthcare, particularly in improving the support available to children and young people with complex health needs. Following his death, it was deemed essential to use these talks to highlight that everyone who contributes to the NHS matters—including young disabled patients, not just those in senior positions.
Who I Am
For those of you who don’t know me, my name is Zoe Picton-Howell. I am Adam’s mother and the founder and director of the Adam Bojelian Foundation. I am also a solicitor specialising in healthcare law and human rights, with a particular focus on children’s rights. My PhD at Edinburgh University Law School examined how senior paediatricians across the UK make best interest decisions, particularly at the end of life, and how they interpret the legal and ethical frameworks guiding those decisions.
I continue to teach at Edinburgh University Medical School and contribute to various expert advisory committees, research panels, and guidance-drafting groups, including statutory guidance. My professional expertise, combined with my personal experiences, has profoundly shaped the insights I will share today.
Adam’s Legacy
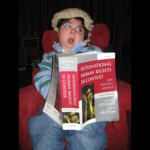
Adam was not only a beloved son but also an extraordinarily talented writer. Due to cerebral palsy, writing was a painstaking process for him—he had to spell out each word using a spell chart or word lists. It could take him weeks to complete a poem. Despite these challenges, his words carried profound impact. Some of you may already be familiar with his blogs and poetry, which won multiple awards, including a Brit Writers’ Award at the age of 10 and a Gold Blue Peter badge.
At age 12, one of his poems, Christmas Gibbons, which tells the delightful tale of gibbons helping Santa deliver presents, was set to music by a now Hollywood-based composer and reached number 2 in the iTunes charts. The Independent on Sunday named Adam as one of the people who brought the most happiness to the UK, while The Scotsman recognised him as one of the key figures who had put Edinburgh on the map that year.
Following Adam’s death, a collection of his poems, Playing with Words, was published and launched at the Edinburgh International Book Festival, a place he loved to visit. Copies are available today, with all proceeds supporting the Adam Bojelian Foundation. A second book, Powerful Poems, which showcases Adam’s advocacy writings, is currently being illustrated and is expected to be available later this year.
As Adam grew older, particularly after our move to Yorkshire, he became a passionate healthcare advocate. His blog, What Does Good Care Look Like?, has been described as transformative within the NHS, as has his poem Leadership. Academics frequently sought his insights, and the Royal College of Paediatrics and Child Health valued his contributions.
The Challenges Adam Faced
Despite his brilliance and achievements, Adam faced immense challenges—not only due to his severe physical disabilities and complex health needs, which meant he spent nearly half his life in hospitals, but also because of the way some consultants dismissed him.
Certain consultants refused to accept that Adam could understand language at all, let alone communicate in an age-appropriate manner. This was despite overwhelming evidence, including his school reports confirming he was top of the class in all subjects, and the fact that BBC journalists could interview him with ease upon first meeting him.
Curiously, it was only specific medical specialisms within paediatrics that questioned Adam’s abilities. Nurses, consultants in more relevant specialisms, allied health professionals, GPs, dentists, teachers, shop staff, café workers, journalists, and even authors he met at the Edinburgh Book Festival never had any difficulty communicating with Adam.
Adam experienced the NHS in all its forms: specialist children’s hospitals, tertiary care centres, district hospitals, intensive care units, high-dependency units, general and specialist wards. He saw the very best of the NHS—but also, sadly, the very worst.
My Perspective as a Lawyer and Mother
As Adam’s mother, I witnessed it all—not only as a parent but also inevitably as a lawyer specialising in children’s healthcare law. At the same time, through my research, I was discussing best practices with senior paediatricians across the UK and helping to shape the very guidelines that should have governed Adam’s care. I observed firsthand the interactions between staff and Adam, between staff and me, between staff and my husband, Paul, and between staff themselves.
These experiences—both inspiring and deeply troubling—form the foundation of what I will share with you today.
The Role of Law in Healthcare
I will begin by sharing key insights from my research with paediatricians and demonstrate how these findings resonate with wider healthcare practice and Adam’s experiences. I will then use the examples from statutes vital in healthcare, to illustrate how the law should not be feared, but rather embraced as a vital tool that ensures optimal patient care, enhances staff well-being, and reduces fear of litigation.
I am aware that some of what I will say may be seen as controversial. However, as Adam’s mother, as a lawyer, an academic, a healthcare educator, and someone who has worked closely with health professionals on numerous committees, I can say with certainty:
Fear of the law is real and widespread among UK health professionals.
This fear is deeply harmful—not just to patients but also to healthcare professionals, families, and carers. It leads to breakdowns in communication and trust, particularly in cases involving complex or long-term health needs.
However, from my perspective as a lawyer, and based on countless discussions with healthcare professionals, I believe this fear is misplaced.
The misunderstanding is not just about legal technicalities in specific situations. It is a fundamental misunderstanding of what the law actually is.
Before I go any further, I invite you to take a moment to reflect. I have provided pens and paper—please take a moment to write down two or three words that come to mind when you hear the word law.
[Pause for delegates to write down their thoughts, if you are reading this after the talk you may wish to do the same]
Many health professionals view the law as a rigid set of rules and restrictions—something that looms over their practice like the sword of Damocles, ready to strike if they step out of line. At best, they see it as a shield, protecting them from lawsuits or criminal liability. As one consultant in my study put it:
“It’s kind of the last resort when you’re desperate… It feels defensive. If the court has decided, it takes the responsibility off you. Nobody is going to charge you with manslaughter or murder the next day. So, for some of us, it’s a kind of protection… but I think it would generally be much better if we didn’t have to go there.”
As a result, the law is often perceived as something relevant only when things go wrong—a tool for self-defence or for patients and families to “get their own back” or seek compensation. This, in my view, is a fundamental misunderstanding—one that leads to poorer healthcare, worse patient outcomes, damaged relationships, and increased stress for professionals.
A more accurate perspective is that law is not about rigid rules; it is about regulating relationships. Law is about good communication and listening. In fact, most legal problems in healthcare could be avoided with better communication. This may sound like an oversimplification, but my research with paediatricians demonstrates just how powerful this perspective can be.
My study, which concluded in 2018, remains highly relevant today. While some promising changes were evident, particularly among junior consultants, increasing pressures on healthcare professionals may have exacerbated the challenges identified. We obviously don’t have time to cover my full thesis—UK Paediatricians’ Medical Decision-Making for Severely Disabled Children: A Socio-Legal Analysis—in detail today, so a lot is left out and a lot is summarised, but for those who are interested in the detail, it is available online via Google Scholar by searching my name, Zoe Picton-Howell.
The Inspiration for My Research
The first event that led me to embark on this PhD occurred when Adam was in hospital in Scotland. He was under the care of a team of consultants, including a neurologist, a respiratory consultant, and an endocrine consultant. Despite being obviously unwell, the respiratory consultant—who had known Adam for years—deemed him well enough for discharge. Yet, both the nurses and I were deeply concerned. Acting on instinct, I left the respiratory ward and sought out Adam’s neurology consultant. Within ten minutes of Adam having been seen by the respiratory consultant, the neurology consultant confirmed Adam was critically ill and needed immediate admission to PICU. In PICU it was confirmed that Adam had severe pneumonia. Thanks to that intervention, Adam received the care he needed and was his well self and back in school within two weeks.
I reflected on this: how could two equally experienced consultants, with the same information and familiarity with Adam, reach such vastly different conclusions? The academic in me was fascinated—what factors were they assessing, and what shaped their judgments?
The second incident or incidents that led to my PhD was observing the number of times medical consultants said things which showed a misunderstanding of the law. Examples that spring to mind include a talk given at a children’s hospital where the speaker told that health professional audience that the Human Rights Act did not apply to children or another occasion where a very senior medical director said when talking again about the Human Rights Act, ‘oh we don’t follow that here’ . It made me realise that there was something seriously wrong in health professionals legal education if people in who should have been living the principles of the Human Rights Act in their daily life had such a fundamental misunderstanding of it. I was therefore curious to learn more about how medical consultants learnt about the law and applied it.
The Study
My research involved 33 paediatricians:
- 10 intensivists
- 9 neurologists
- 2 respiratory consultants
- 12 paediatricians from other specialties
Nine of these doctors participated in in-depth interviews. Their qualifications spanned from the 1960s to 1998, representing all NHS regions except Northern Ireland, Trent, and Eastern. Some had also trained and worked abroad. Notably, none had worked with Adam or me to maintain objectivity.
A key observation was that participants were likely those with a particular interest in the subject, meaning they were not necessarily representative of all paediatricians. However, they all routinely made end-of-life decisions for disabled children and were often in influential roles, such as department heads or members of regional and national committees, so influencing others.
Interestingly, more doctors in my study than statistically expected identified as parents of disabled children. Their perspectives stood out. While doctors with disabled siblings did not show the same pattern, those who were parents of disabled children were more positive and supportive toward parents, saw greater potential in disabled children, and viewed them as more active participants in decision-making.
The Role of Legal Consciousness
To analyse how paediatricians engaged with the law, I applied the Legal Consciousness Framework, which examines how people experience and interact with the law in everyday life. It identifies three categories:
- Before the Law – The law is seen as a distant, formal system that ensures fairness. Those in this category believe the legal system will function properly if needed.
- With the Law – The law is viewed as a tool to be navigated and used strategically, often by those who understand its complexities.
- Against the Law – The law is seen as oppressive, unfair, or difficult to navigate, leading people to resist or avoid it altogether.
This framework is particularly useful in healthcare, where legal consciousness can be both individual and collective. Medical training itself is a process of socialization, shaping how doctors interpret law and ethics. As influential legal scholar Ian Kennedy argued, doctors make legal and ethical decisions they are not formally trained to make.
Understanding Paediatricians’ Legal Context
Paediatricians operate within a complex legal and professional framework, including guidance from the General Medical Council, the Royal College of Paediatrics and Child Health, NICE, and jurisprudence from English and Scottish courts. As NHS employees, they must also comply with the Human Rights Act 1998 and relevant UN human rights treaties.
Beyond legal structures, doctors are deeply embedded in medical, paediatric, and NHS cultures, each with its own norms and values. Even within a single hospital, these cultures can vary significantly between wards, specialties, and peer groups. Public perception often assumes uniformity in NHS care, but as one consultant in my study starkly put it:
“What I worry about is equity. If you show up on a Wednesday in May, you get one set of specialists. If you show up on a Thursday in April, you get a different set—and that determines your outcome.”
This echoes findings from high-profile inquiries, such as the Bristol Royal Infirmary Kennedy Inquiry and Mid Stafford Francis Report, or the findings of the Learning Disabilities Mortality Review programme, all of which highlight how professional culture, values, and attitudes directly impact patient care and staff well-being and something we witnessed throughout Adam’s life and even death.
Paediatricians, like all healthcare professionals, exist in a landscape shaped by overlapping cultures—some complementary, others competing. Their legal consciousness is influenced by their education, personal experiences, faith, politics, and regional backgrounds. These factors shape not only how they perceive the law but also how they apply it in practice.
Before directly asking the consultants about law and ethics, I first explored how they understood certain commonly used terms and phrases, such as ‘prognosis’, ‘futility’, ‘quality of life’, and ‘cognitive ability’. I did this because a consultant’s interpretation of these terms influences how they apply the law and follow professional guidance.
What I found particularly interesting was the lack of consensus among consultants, even for a term as fundamental as ‘prognosis’. Their definitions varied widely, including descriptions such as:
- ‘Trajectory of illness’
- ‘Severity’
- ‘Pain and discomfort’
- ‘Current clinical knowledge about the condition’
- And, perhaps unexpectedly, one consultant described it as ‘parental aspiration’.
Clearly, when there is no agreement on what is being assessed, it is difficult to apply strict rules and regulations.
There was also significant variation in how consultants weighted different factors when making end-of-life decisions. Despite coming from a relatively narrow spectrum of society and the medical profession, the consultants in my study demonstrated diverse perspectives on what should be considered and how much weight each factor should carry. Some broad trends emerged within sub-groups; for example, consultants who qualified in the 1990s appeared more inclined to consider futility and a child’s perceived quality of life, despite the lack of consensus as to what these terms mean, in their best-interest decisions, whereas those who had qualified decades earlier placed less emphasis on quality of life.
Of all the factors, quality of life stood out for the diversity of ways it was interpreted and applied. Many consultants seemed to use it as a proxy for a child’s best interests, drawing on a wide range of clinical and non-clinical (welfare) considerations.
My study suggested that, in assessing a child’s best interests, consultants tended to place greater weight on non-clinical factors—such as quality of life—than on strictly clinical ones. In my study, clinical factors were defined as those based on direct observation and treatment by a health professional, whereas non-clinical factors included, according to the consultants, considerations such as whether a child was happy at school or their relationships with others.
This brings us back to Ian Kennedy’s critique, which remains highly relevant. He argued—rightly, in my view—that medical professionals often assess non-clinical factors beyond their expertise, sometimes making prejudicial assumptions rather than consulting those with direct experience. In some cases, this includes failing to consult the patient themselves, even when appropriate.
Indeed, as I mentioned at the beginning of my talk, Adam’s experience illustrates this problem clearly. Many paediatricians wrongly assumed he could neither understand nor communicate, simply because of his physical impairment.
As mentioned earlier, I was also interested in the legal and ethical education of consultants. Every clinical decision has a profound impact on a patient’s rights—whether it is something as straightforward as consenting to be touched or to remain in hospital, or as complex as undergoing highly invasive surgery or facing the withholding or withdrawal of treatment, which may ultimately lead to death. Given the gravity of these decisions, a doctor’s understanding of the legal and ethical implications of their daily practice is crucial. I wanted to explore how medics acquire this knowledge and from whom.
Formal education and training in law and ethics were notably lacking. Only nine doctors (27%) in my study reported receiving any legal or ethical education during medical school. For all but two of them, this education was minimal—typically a single lecture. The remaining 73% reported having received no such education at all. Notably, the two doctors who received more than minimal training had studied in Scotland and mainland Europe.
The gaps in education persisted beyond medical school. Seventeen doctors (52%) reported having had no further training in law, rights, or ethics since qualifying. This is particularly significant given that all participants in my study were paediatricians. The UK government has repeatedly assured the UN Committee on the Rights of the Child that all professionals working with children in the UK receive education and training on the Convention on the Rights of the Child. My findings suggest that this may not be the case. In total, my study found that 48% of the paediatricians surveyed had received no formal training or education in law, rights, or ethics at any stage, despite making daily decisions that affect their patients’ rights.
Three doctors had sought out master’s-level courses in healthcare law and ethics, but their motivations were unclear. Were they, as legal consciousness theory suggests, arming themselves with the law as a sword, protecting themselves with it as a shield, or simply striving to provide the best possible patient care? My data did indicate that more recently qualified doctors were more likely to have received some education in law and ethics compared to those who qualified earlier. This suggests that the situation may be improving, but at the time of my study, almost half of the doctors responsible for best-interest decisions had received no legal or ethical education.
A particularly striking finding was that even when training in law and ethics was provided, it was usually delivered by a medic rather than a lawyer. The common justification for this approach is that only medics can truly understand the context in which clinical decisions are made. However, this misunderstands the role of most lawyers, who immerse themselves in their clients’ professional environments to understand the context of their decisions. The concern, as Kennedy has previously noted, is that doctors are not trained in law. While some complete a master’s course in healthcare law and ethics, this provides only limited legal expertise. To draw a comparison from my own life, when Adam was young I completed a masters in alternative communication for children, but this did not furnish me with the expertise to teach others about the subject, despite being an experienced university tutor.
To draw another comparison, during Adam’s life, I gained significant knowledge about epilepsy—not only from Adam’s day-to-day experience but also from serving on committees such as confidential child death reviews, where multiple cases were examined, and from reading relevant research papers. However, despite this knowledge, it would not be acceptable for me to teach medical professionals about epilepsy, as I am not a trained and experienced medical doctor and I don’t think any doctor would accept clinical training from me. Likewise, it is problematic for doctors without formal or limited legal training to be the primary educators on law and ethics.
In my view, legal and ethical education for medics should be jointly delivered by both doctors and lawyers, ensuring that training benefits from the expertise and perspectives of both professions. Indeed, several doctors in my study who had received training in law and ethics from medics alone felt that it was overly defensive and biased, focusing exclusively on the law as a shield with no consideration of the law from the patient’s perspective or as a tool for patient advocacy. Indeed, several suggested the education they did receive increased their sense that law was something to be feared.
Another key finding from my study was that consultants who had completed some legal education were often perceived by their colleagues as having far greater legal expertise than their actual level of training warranted. These doctors were frequently regarded as legal experts, entrusted with educating their peers on legal matters, deferred to in situations involving legal questions, and appointed as heads of ethics committees.
One doctor in particular, who was eager to discuss the law in great depth during their interview, was keen to demonstrate their knowledge of case law and statutes. However, from a legal perspective, much of what they cited reflected misunderstandings of the law. Despite this, they appeared to embrace the law and draw both personal and professional empowerment from their perceived expertise. They seemed to gain status and admiration from colleagues and suggested that legal knowledge provided them with authority over junior doctors, patients, and families. Based on this, I proposed an additional category of legal consciousness: law as kudos.
I suggested that this category of legal consciousness is likely to be found among elites—those who have easy access to legal education and who already hold positions of respect and power. While studying law and ethics may provide individuals from marginalized groups with a sense of personal empowerment, unless they formally enter the legal profession, it seems less likely that they would be able to leverage their legal knowledge to enhance their professional status in the same way. In contrast, the doctors in my study who had undertaken even a relatively short course in law were ascribed significant legal expertise by their peers—an example of the relational nature of legal consciousness. While these doctors were viewed as legal authorities within the medical community, they would likely not be perceived as such by lawyers.
This raises an important question: does legal education matter, particularly when so many doctors have had little or none at all? Do those who have studied law and ethics act more lawfully or provide better patient care?
The answer is perhaps counterintuitive. However, my findings may offer insight into why some doctors choose to pursue legal education, such as a master’s course in healthcare law and ethics. In my study, I examined whether doctors who had undertaken legal training approached end-of-life decisions differently from those who had not. I specifically asked participants about the relevance of law and ethics to their best interest decisions. Strikingly, none of the doctors explicitly mentioned best interests or a similar concept in response, despite best interests being the central legal and ethical framework for end-of-life decision-making. Only four doctors (12%) had previously identified best interests as a factor in their decision-making, suggesting that many did not recognize it as a legal construct.
Notably, 60% of the doctors in my study made no reference to best interests or a similar concept—such as balancing benefits and burdens—at any point in their survey responses or discussions. Additionally, 14 doctors (42%) stated that as long as they did not break the law, the law had no relevance to their decision-making. This reflects a perception of the law as something external, influencing practice only when problems arise, rather than as an intrinsic part of clinical decision-making.
Overall, doctors who had received legal education or training did appear to conceptualize best interest decisions for disabled children differently from their colleagues who had not. However, whether this difference was a direct result of their legal training or whether doctors with a particular decision-making approach were more likely to seek out legal education remains unclear. One striking finding was that doctors who had studied law tended to fear it more than those who had not.
At the outset of this talk, I noted that fear leads to poor patient care and negatively impacts staff well-being. The doctors in my study, particularly those who had studied law, described precisely this fear. They reported taking steps to protect themselves, avoid litigation, and, in their words, prevent losing their licence—rather than focusing on acting in the patient’s best interests. This anxiety was severe, with some doctors describing, deep moral uncertainty, sleepless nights due to their concerns about the legal implications of their decisions, or confusingly from my perspective as a lawyer saying they took decisions they knew to be wrong to avoid being sued or sanctioned by the GMC.
When each doctor’s decision making was mapped to how the jurisprudence of the Court says best interests decisions should be made, the doctors who saw themselves has having legal expertise following their studies, tended to view themselves as the sole decision-maker, the experts in law, medicine and the child, making decisions, contrary to the law, unilaterally rather than consultatively.
In contrast, doctors who were not overly focused on legal rules—those who did not see the law as particularly relevant to their work—were, counterintuitively, the ones whose decision-making aligned most closely with legal requirements. They routinely consulted widely, involved children in decisions where possible, carefully balanced benefits and burdens, and engaged in broad discussions to ensure all perspectives were considered. Several doctors in this group—whom I termed softliners, in contrast to the hardliner label one doctor in the legalistic group had given herself—expressed that they did not see themselves as decision-makers. Instead, they viewed their role as coordinators, responsible for gathering and balancing information to determine the best course of action. This approach closely reflects how English case law on children’s best interests and the Mental Capacity Act’s framework for those over 16 define the best interest decision-making process.
Ultimately, it may be misleading to speak of a singular ‘best interest decision’ at all. Disagreements are inevitable—not, as the media often portrays, between doctors and parents, but, as my study revealed, between consultants from different specialisms, each bringing their own perspective on what is best for the child. The law does not demand the imposition of a single ‘correct’ decision but instead requires a best interest process—one that involves the broadest possible consultation to ensure all relevant information and viewpoints are considered before taking potentially irreversible steps.
This raises an important question: does teaching law to health professionals unintentionally contribute to the very fear that harms both patients and staff well-being, eroding trust rather than strengthening it? At first glance, my study might suggest that it does. However, my broader research leads me to believe otherwise. One key observation is that nurses who have studied law tend to understand and apply it more effectively—aligning with how the courts intend—compared not only to nurses who have not studied law but also to doctors who have.
I believe this difference may be explained by my new legal consciousness classification. In the hierarchy of healthcare professionals, consultants hold elite status in a way that nurses do not. Studying law may not carry the same prestige for nurses as it does for consultants, which raises the question of whether their motivations for legal education differ. My experience suggests that when law is understood and applied correctly, it enhances both patient care and staff well-being. The key is in how it is taught: not as a weapon—a sword to attack or a shield to defend—but as a practical tool to support better patient care.
So let’s look at some examples to understand how law can be wrongly used enhancing a health professional’s fear and leading to less than optimum patient care and then look in each case how when properly understood the same law can be used as a tool to both improve patient care and health professional well-being
Let’s turn first to the Mental Capacity Act 2005,as an example:
Let’s take this scenario:
Scenario:
A 90-year-old woman with dementia is admitted to the hospital with pneumonia. She is confused and unable to understand the risks and benefits of treatment. The medical team must decide whether to administer intravenous antibiotics and whether she should stay in the hospital or be treated at home with support.
A medical consultant for example, who is very fearful of the law might wrongly apply the Mental Capacity Act 2005 (MCA) in several ways:
- Overly Defensive Decision-Making
Instead of assessing the patient’s best interests carefully, they may default to the most conservative or “legally safest” option—admitting the patient to the hospital—without fully considering whether this is the least restrictive and most appropriate approach. Fear of being sued or investigated might lead them to prioritize defensive medicine over patient-centred care.
- Rigid Interpretation of Capacity
- The consultant might assume that dementia automatically means the patient lacks capacity without conducting a proper assessment under Sections 2 and 3 MCA. Wrongly assuming incapacity due to living with the a particular condition is, in my experience, the most common error made by health professionals about the MCA.
- They could also fail to recognize that capacity is decision-specific and may fluctuate, leading them to dismiss any attempts by the patient to express a preference.
- Failure to Consider the Patient’s Wishes and Best Interests Properly
- Out of fear of legal scrutiny, they might over-rely on what they believe is a “standard” or “safe” decision rather than following the structured best interests process.
- They may focus too much on medical opinions and fail to give enough weight to the views of the family, carers, or the patient’s known prior wishes.
- Instead of weighing the least restrictive option, they might insist on hospital treatment even if home care is more appropriate.
- Misuse of ‘Best Interests’ to Justify a Defensive Decision
- Rather than genuinely considering all relevant factors, they might justify a decision by saying, “It’s in her best interests” without thorough consultation. In my experience, medics saying something is in a patient’s ‘best interests’ to close down discussion, without any proper consideration of the patient’s best interests is another common error and indeed something we saw first hand at the end of Adam’s life.
- This can lead to paternalistic decisions that overlook the patient’s autonomy and past preferences.
- Failure to Engage with the Wider Team
- A fearful consultant might make the decision in isolation, without properly involving the multidisciplinary team, family, or carers, or the patient when appropriate, out of concern that differing views could lead to legal challenges.
- This lack of consultation increases the risk of making a decision that is legally questionable and may later be challenged.
- Unnecessary Court Referral
- While Court of Protection involvement is sometimes necessary, a consultant who is overly anxious about the law might refer the case to court unnecessarily, delaying treatment and causing additional distress to the patient and family.
- The MCA is designed to empower clinicians to make well-reasoned best interests decisions without excessive legal intervention, provided they follow the correct process.
Conclusion
Fear of the law can lead to overly restrictive, defensive, and paternalistic decisions that ultimately fail to serve the patient’s best interests. The correct application of the MCA provides a structured, legally sound approach that balances legal compliance with ethical and compassionate decision-making.
This is sadly the approach too often taken, but the Mental Capacity Act was enacted by Parliament to:
- Empower individuals to make their own decisions where possible.
- Protect those who lack capacity by providing a clear framework for decision-making.
- Clarify who can make decisions on behalf of someone who lacks capacity and in what circumstances.
- Ensure decisions are made in the person’s best interests and in the least restrictive manner possible.
- Create safeguards to prevent abuse, including the establishment of Lasting Powers of Attorney, the Court of Protection, and Independent Mental Capacity Advocates (IMCAs).
The MCA was designed to strike a balance between autonomy and protection, ensuring that individuals retain as much control as possible while providing support when necessary.
So, using the Act correctly:
- Assessing Capacity (Section 2 & 3 MCA)
- The team assesses whether the patient can understand, retain, weigh, and communicate information about her treatment.
- They determine that she lacks capacity to decide about her hospital stay and antibiotic treatment, remembering the presumption in the statute that an individual does have capacity.
- Best Interests Decision (Section 4 MCA)
- The doctors and nurses do not assume what is best but instead follow a structured best interests process:
- They consult family members who know the patient’s wishes, and the patient as far as possible, giving the patient the assistance needed to participate as far as possible.
- They consider past and present wishes, such as whether she had expressed a preference for home care.
- They speak to her GP, carers, social workers and allied health professionals to understand how she copes at home.
- They assess whether hospital admission is the least restrictive option.
- Minimising Restriction (Section 1(6) MCA)
- The team decides that the best approach is to treat her at home with community support, as this aligns with her prior wishes and is less distressing than hospital admission.
- They ensure she has appropriate support (community nurses, home visits, and emergency contact plans).
Benefits for Patient Care
- The patient receives care tailored to her best interests, rather than a one-size-fits-all hospital admission.
- Her dignity, autonomy, and comfort are respected.
- The structured MCA process ensures all relevant perspectives are considered, reducing the risk of inappropriate or distressing interventions.
Benefits for Practitioner Well-being
- Reduced Fear & Anxiety: By following the MCA, practitioners avoid making rushed or defensive decisions out of fear of legal repercussions.
- Confidence in Decision-Making: Using the best interests framework reassures practitioners that they are acting lawfully and ethically.
- Reduced Conflict & Stress: Consulting widely and involving family reduces disputes and complaints, making decision-making less stressful.
- Ethical Satisfaction: Knowing they have respected the patient’s rights and dignity improves job satisfaction and emotional well-being.
So, we can see here applying the Mental Capacity Act 2005 as intended by Parliament, rather than defensively ensures better patient care while also supporting practitioners‘ legal, ethical, and emotional well-being.
Let’s take another example the Mental Health Act 1983 – which is currently under review by Parliament, and this scenario:
Scenario: Compulsory Admission Under Section 2 for Assessment
A 35-year-old man with severe schizophrenia stops taking his medication, leading to hallucinations and delusions that make him a danger to himself and others. He refuses voluntary admission, believing the hospital staff are part of a conspiracy against him. His family and community mental health team grow increasingly concerned as his condition deteriorates.
A health professional acting defensively:
- Overuse of Detention ‘Just to Be Safe’
- A doctor fearing legal repercussions may section the patient too quickly without fully exploring alternative options, such as community treatment.
- They might detain the patient under Section 3 instead of Section 2, unnecessarily committing them for a longer period when further assessment could suffice.
- Instead of seeking voluntary engagement first, they may default to detention out of fear of being blamed if something goes wrong.
- Ignoring the Least Restrictive Principle
- The MHA Code of Practice emphasizes the least restrictive option. A defensive clinician may ignore this, opting for hospital detention instead of intensive community support out of concern that allowing him to stay in the community could result in professional scrutiny if an incident occurs.
- Even within the hospital, they might use seclusion or restraint more readily than needed, prioritizing legal protection over patient dignity.
- Failure to Consider the Patient’s Rights
- The patient has the right to an Independent Mental Health Advocate (IMHA) and to appeal their detention, but a defensive clinician may:
- Discourage or delay access to an IMHA, fearing legal challenges.
- Withhold information about appeal rights to prevent a tribunal from overturning detention.
- May not even be aware of these rights or how the patient can access them.
- Overuse of Section 5(2) for Convenience
- Section 5(2) allows a doctor to hold a voluntary patient in hospital for up to 72 hours while awaiting a full MHA assessment.
- A fearful clinician might use Section 5(2) unnecessarily, preventing the patient from leaving, even when there is no immediate risk, simply to avoid professional scrutiny.
- Avoiding Responsibility by ‘Passing the Case Up’
- Rather than making a clear decision, a fearful doctor may over-refer to senior colleagues or legal teams, delaying urgent intervention.
- They might overuse Court of Protection referrals, fearing legal consequences if they make the decision themselves, even when the MHA already provides a lawful framework.
Conclusion
A health professional acting out of fear rather than professional judgment may misuse the Mental Health Act by defaulting to detention, ignoring least restrictive options, limiting patient rights, or delaying urgent care through excessive referrals. The MHA is intended to protect patients’ rights while ensuring necessary care, not to shield professionals from legal scrutiny at the expense of the patient’s best interests.
But:
Parliament intended to provide a legal framework for the assessment, treatment, and rights of individuals with mental disorders while balancing patient autonomy, public protection, and clinical necessity. The Act was designed to:
- Ensure appropriate care and treatment for individuals with serious mental health conditions, particularly those who may not seek or accept treatment voluntarily.
- Provide legal authority for compulsory detention and treatment in specific circumstances where an individual’s mental disorder poses a risk to themselves or others.
- Safeguard patient rights by setting out clear procedures for detention, appeals, and review by tribunals and independent bodies.
- Balance individual liberty with public protection, ensuring that compulsory treatment is used only when strictly necessary and proportionate.
- Regulate the roles of professionals (such as Approved Mental Health Professionals and Responsible Clinicians) in decision-making regarding detention and treatment.
The Act was largely influenced by concerns over patient rights and civil liberties while acknowledging the need for compulsory treatment in cases of severe mental illness. It replaced earlier legislation to reflect evolving medical, ethical, and legal perspectives on mental health care.
How the Mental Health Act can ensure the Best Possible Care
- Section 2 of the MHA 1983 allows for the patient’s compulsory admission to hospital for up to 28 days for assessment and treatment, provided that:
- Two doctors confirm he has a mental disorder requiring hospital treatment.
- An Approved Mental Health Professional (AMHP) agrees that detention is necessary for his health, safety, or the protection of others.
- Immediate Benefits for the Patient:
- Access to treatment: He can receive appropriate antipsychotic medication and psychological support, improving his symptoms.
- A structured care plan: The clinical team can assess his condition, stabilize him, and plan for his long-term care.
- Protection of his rights: The Act provides legal safeguards, such as the right to appeal and regular independent review.
How This Improves Staff Well-being:
- Reduces moral distress: Healthcare staff often experience ethical dilemmas when a patient refuses necessary treatment. The MHA provides a clear legal framework, ensuring decisions are made lawfully and ethically.
- Enhances safety: Staff can intervene before a crisis escalates, reducing the risk of violence or self-harm, which can cause trauma to both the patient and the healthcare team.
- Supports a collaborative approach: The requirement for multi-professional involvement (doctors, AMHPs, nurses, and family where possible) helps staff feel supported in their decisions, reducing fear of legal repercussions.
- Long-term job satisfaction: Seeing patients recover and regain stability reinforces a sense of purpose and professional fulfillment, preventing burnout.
By balancing patient rights with the need for care, the Mental Health Act 1983 ensures timely intervention, protects staff from ethical and legal uncertainty, and ultimately promotes better outcomes for both patients and practitioners.
And finally lets look at an example from the Human Rights Act 1998:
Scenario: Ensuring Dignity and Appropriate End-of-Life Care (Article 8 & Article 3)
An elderly patient with advanced motor neurone disease (MND) has lost the ability to communicate verbally and is nearing the end of life. He expresses, through previous written statements and communication aids, that he does not want invasive life-prolonging treatment, such as mechanical ventilation. However, his family disagrees and insists that all possible interventions should be pursued. The medical team feels conflicted about whether continuing treatment is in the patient’s best interests.
If those treating this patient act out of fear of the law:
- Fear of legal action from the family may lead the medical team to override the patient’s advance decision whether to provide life-prolonging treatment or withdraw it against the patient’s clearly expressed wishes.
- This disrespects the patient’s right to autonomy and bodily integrity, violating Article 8.
- Unnecessary Prolongation of Suffering Due to Defensive Decision-Making (Violation of Article 3 – Right to Be Free from Inhuman or Degrading Treatment)
- Doctors may fear accusations of negligence if they withdraw life-prolonging treatment, even when it is causing suffering with no clinical benefit.
- Continuing mechanical ventilation or aggressive interventions against the patient’s prior expressed wishes could prolong distress, pain, and indignity.
- The European Court of Human Rights (ECtHR) has ruled that subjecting a patient to treatment they find degrading or distressing can breach Article 3.
- Failing to Act Due to Fear of colleague or Family Backlash (Violation of Article 2 – Right to Life, But Also a Misinterpretation of This Right) and also avoiding discussions with colleagues, patients and family members for fear this will lead to disagreements. The European Court of Human Rights has made clear that the withholding or withdrawing of treatment after full and proper assessment of the correct factors which results in a patient’s death is not a breach of Article 2 of the European Convention.
- Avoiding Responsibility by Seeking a Court Order Unnecessarily
- Instead of making a clear, well-reasoned clinical decision, a fearful doctor may refer the case to the Court of Protection too quickly, fearing criticism or legal consequences.
- While some cases require court involvement (e.g., if an advance decision is disputed), an unnecessary court referral:
- Delays decision-making, prolonging suffering.
- Passes responsibility to the legal system instead of following clear legal and ethical principles.
- May be financially and emotionally burdensome for all involved.
- Excluding the Patient’s Voice from the Decision-Making Process
- Out of fear of conflict with the family or colleagues, the medical team might focus solely on the family’s/colleagues’ demands and fail to properly advocate for the patient’s expressed wishes.
- Even if the patient cannot speak, their previously recorded preferences should take precedence under the MCA and HRA.
- Article 8 protects the right to personal autonomy, which should not be ignored due to family pressure or professional anxiety.
Article 14: It is well documented that patients living with disability are routinely denied access to care and treatment based on prejudicial assumptions about their quality of life, the doctors in my study talked about this a great deal, some raising concerns that their consultants colleagues routinely did this, and others openly discussed how they did so for example, PICU consultants saying they would never admit a child with cerebral palsy to their unit, rather than individually assessing each child. Article 14 prohibits an individual being discriminated in any of their European Convention Rights.
The Human Rights Act is however, designed to protect patients from all these very abuses, ensuring that end-of-life care is guided by dignity, autonomy, and compassion—not fear-driven decisions that prioritize legal self-protection over the patient’s best interests.
In contrast:
How the Human Rights Act 1998 Ensures the Best Possible Care
- Article 8 (Right to Private and Family Life):
- Protects the patient’s autonomy, dignity, and right to make decisions about their own body and treatment.
- Requires clinicians to respect the patient’s previously expressed wishes, ensuring treatment decisions align with what the patient would have wanted.
- Article 3 (Prohibition of Inhuman or Degrading Treatment):
- Prevents unnecessary suffering by ensuring patients are not subjected to prolonged, distressing, or non-beneficial treatment.
- Guides doctors in making clinically and ethically sound decisions, balancing the duty to preserve life with the duty to prevent suffering.
- Article 2 the Right to Life
- Ensures an individual’s life is protected by the state and that in certain circumstances, deaths are properly and full investigated.
- It does not prevent the withdrawal or withholding of life saving or life extending treatment, when this has been properly and fully assessed, without prejudicial bias.
- Article 14 prevents a disabled patient being refused treatment and care based on prejudicial assumptions about the disability and their quality of life.
How This Improves Health Professional Well-being
- Reduces ethical distress: The legal clarity provided by the Human Rights Act ensures that doctors and nurses do not feel pressured to administer unnecessary or harmful treatment.
- Prevents conflicts with families and colleagues: By grounding decisions in human rights law, healthcare professionals can explain that they are following a legal and ethical framework, rather than making arbitrary decisions.
- Enhances job satisfaction: Knowing they are acting in the patient’s best interests, while respecting their dignity, reinforces a sense of professional integrity and well-being.
- Provides legal protection: Healthcare professionals can feel reassured that their decisions are legally defensible, reducing fear of litigation.
By applying the Human Rights Act 1998, health professionals can ensure that patient care is ethical, lawful, and person-centred, while also protecting their own well-being from undue stress, moral injury, and legal uncertainty.
In each of these examples, we see how a correct understanding of the law transforms it from a source of fear into a tool that enhances both patient care and practitioner well-being. When the law is misinterpreted or approached defensively, it can create unnecessary stress for health professionals and erode trust in decision-making. However, when taught and applied in the way Parliament intended—focusing on rights, dignity, and ethical decision-making—it empowers clinicians to provide better care with greater confidence.
This brings us back to a key question: does teaching law to healthcare professionals cause harm? The answer is not in the teaching itself but in how the law is framed. If taught as a rigid set of risks to avoid, it fuels defensive practice, anxiety, and mistrust. But if we shift the focus to law as a supportive framework, as the regulation of relationships, encouraging good communication—one that guides ethical, patient-centred care—then it becomes a powerful ally rather than a burden.
When health professionals receive proper legal education, they:
✔ Make confident, patient-centred decisions without unnecessary fear.
✔ Respect patient rights rather than practising defensively.
✔ Feel less anxious about legal repercussions, improving job satisfaction.
✔ Reduce conflicts and unnecessary court involvement.
✔ Challenge misinformation and resist pressure from those who misunderstand the law.
One way to achieve this is by ensuring that legal education for health professionals is delivered in collaboration with lawyers who have expertise in healthcare and also many have suggested also experienced patients. By working together, clinicians and legal experts can bridge the gap between law and practice, fostering confidence, clarity, and compassionate care. The challenge, then, is not whether we should teach law to healthcare professionals, but how we ensure they learn it in a way that truly supports both them and their patients.
Thank you
This is the 2025 Adam Bojelian Memorial Talk delivered on 31st March 2025 by Dr Zoe Picton-Howell, a solicitor, an expert in healthcare law and ethics and Adam’s mother. Thanks to everyone who attended the talk and shared your valuable insights. Thank you also to Horizon Leeds for hosting us.
Dr Zoe Picton-Howell retains all intellectual property rights in this talk but grants a licence for it to be used for educational and training purposes. Prior permission for any other use should be sought via [email protected] from Dr Picton-Howell for its use and use of the accompanying YouTube video in any other way.
Back to About AdsTalks
Forward to AdsTalk24 with Charlie Jones

